Written by Dr. Quinn Henoch
Patellofemoral Pain Syndrome (PFPS) is a common ailment in the athletic population. Incidence rates among adolescent and young adult athletes can exceed 25%, with females more likely to experience it, than their male counterparts.

PFPS is typically characterized by a dull, achy pain around or behind the kneecap that begins without a known incident, and is aggravated by anything that loads the knee while it is flexed – squatting, step up/stairs, running, jumping and even prolonged sitting. Among runners, it is the most common overuse injury, and unfortunately, becomes a chronic issue for many that experience it, regardless of the preferred activity. Needless to say, this can have a huge impact on training.
**Disclaimer**
PFPS is an actual medical diagnosis and should be made by a medical professional. Self diagnose at your own risk. We will simply refer to general patellofemoral pain (PFP) from here on.
There are numerous research studies attempting to explain the causes and most effective treatments for this mysterious, but all too common ailment, including the most recent consensus statement from the British Journal of Sports Medicine.
Like many research topics, the information available on PFP seems to be, at times, contradictory and unclear. The purpose of the article is to translate what seems like a jumbled mess of research into something reasonably digestible and applicable to the athlete or coach, regarding the causes and possible treatment of PFP.
Causes (Or Effects) of PFP
The etiology (cause) is multifactorial. Basically, we do not know exactly what causes it, and several different elements are at play. There is not a sure fire injury mechanism to PFP the way there is with something like a knee ligament tear, and PFP can be present with or without structural wear and tear of the cartilage behind the knee cap. The insidious (gradual and subtle) onset is what makes it such a challenging and confusing issue to deal with; but here is what we have so far:
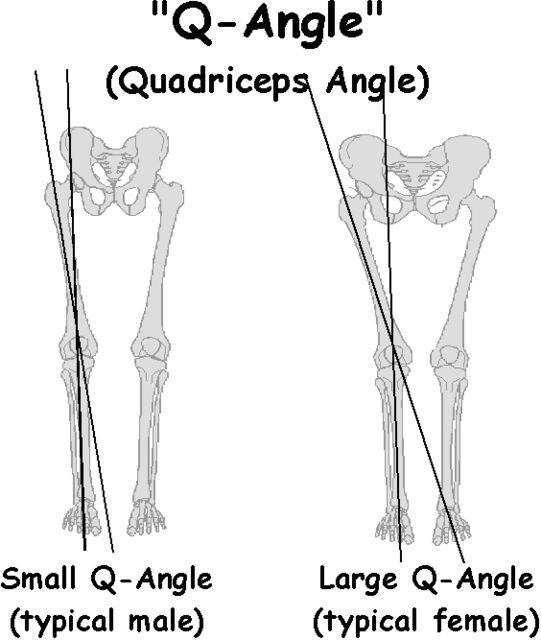
- Static Structural Alignment: Q-Angle (Quadriceps Angle)
The Q-angle is measured from the bony prominence in the front of the hip to the kneecap. Women typically have a larger Q-angle. Combine that with the fact that PFPS occurs more frequently in females, and studies that have shown a relationship between a large Q-angle and increased force through the knee, and it is reasonable to assume that static Q-angle is a potential risk factor for PFP.
 HOWEVER, more recent literature has shown that Q-angle is not a risk factor. So in other words, static Q-angle alone does not predict your chances of developing PFP.
HOWEVER, more recent literature has shown that Q-angle is not a risk factor. So in other words, static Q-angle alone does not predict your chances of developing PFP.
Other research has shown certain abnormalities in the way that the patella tracks with the femur is associated with cartilage damage; however, this has not been shown to be predictive of PFP either. People with seemingly fine patellar tracking and no cartilage damage can develop it just as commonly.
**Take Home Point**
- Not that any of you would do this, but telling athletes or clients that they are at risk for knee pain in the future because of the shape of their hips or structure of their joints, is probably not the best idea. I have experienced a specific case in which a young woman, pain-free at the time, was warned by a professional that squatting may be bad for her knees because of her Q-angle (“wide hips”). 3 months later she had patella-femoral pain. I am not saying planting that seed caused her pain, but it sure as hell did not help.
- Altered Kinematics
So we move on from static alignment to dynamic alignment. Here, we begin to see trends; however, at times these trends seem inconsistent and contradictory. Of course they do. It’s peer-reviewed literature.
Those experiencing chronic (3 months or more) PFP frequently demonstrated altered kinematics in activities such as walking, running, squatting, and landing from a jump when compared to healthy control groups. Examples include:
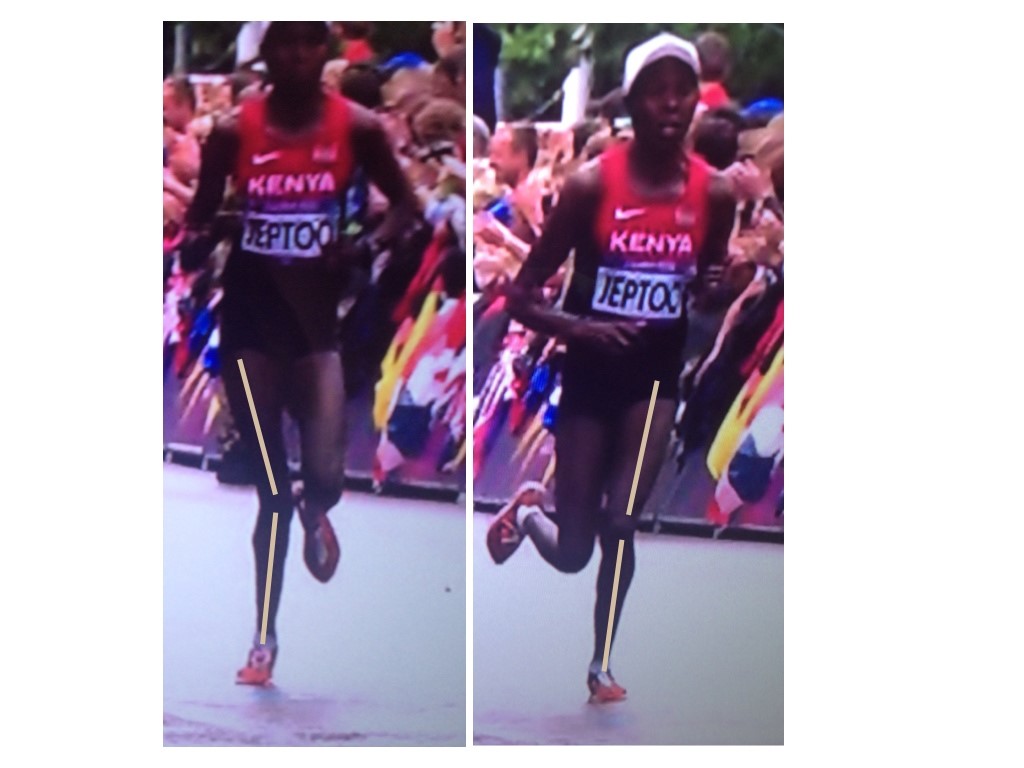
- Higher peak knee valgus (knee caving in) on the stance leg during running in those with PFP, which increased with exertion and fatigue.
- Greater amounts of trunk lean, pelvic drop, hip adduction and knee valgus during single-leg squatting and repetitive single leg jumps.
- Greater hip internal rotation moments during running, step-down activities, and depth jumps.
- Greater rear-foot eversion (heel goes out) during walking
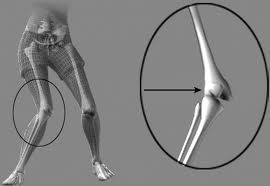
We are probably very familiar with these types of examples. Knee caves in/foot collapses during dynamic activity, which increases the dynamic Q-angle and presumably increasing contact pressure between the patella and femoral condyles. Ok, so when the knee repeatedly caves in, this causes PFP. Not so fast…
Those with PFP also demonstrated movement patterns such as these:
- Increases in hip adduction without increases in hip internal rotation
- Increased hip internal rotation without hip adduction
- Increased hip abduction upon impact when running – so basically the complete opposite
- No increases in knee valgus, but simply inconsistent knee position from rep to rep or stride to stride
- Reducing motion at the trunk, hip, and knee in ALL planes during running stride – seemingly as a protective mechanism.
Clearly those with PFP move differently. Sometimes they move more than normal, in one plane, sometimes less than normal. Sometimes fatigue increases alterations in mechanics; sometimes it seems to actually cause a decrease in alteration, as the individual tries to compensate. The complexity is compounded with variables such as pain onset & perception, training age and experience, etc. Yikes.
IS THIS CAUSE OR EFFECT? Do the altered mechanics cause the pain or does the pain cause the altered mechanics?
We know from pain research that movement patterns change when pain is present, which is consistent with the findings above. We move differently when we are hurt. As for as kinematics being the cause, one study showed that increased hip adduction during running stride was a common trait among female runners that eventually developed PFP (15 out of 400). Neither hip internal rotation or ankle eversion (collapse) was significantly related to those who eventually developed PFP. In another study, 240 healthy young female basketball players were at twice the risk of developing PFP if they demonstrated increased knee valgus forces upon landing from a jump.
Certainly this is not enough evidence to say one particular movement pattern is a cause of PFP, but it certainly lends credence to the idea that certain positions and movements seem to be a bit riskier than others; at least in certain populations. We must keep in mind that those two studies looked at adolescent female athletes who participated in specific activities (running and basketball) only.
We likely see such varied movement strategies in PFP literature because of the unpredictable nature of chronic pain, as well as the variance in patient population (male vs female, adolescent vs adult) and testing methods that were used.
**Take Home Points and Soap Box**
- As an athlete, avoid training compensatory patterns (no matter what they are), if at all possible. This means, that if you are experiencing chronic symptoms, similar to that of PFPS, and those symptoms alter your movement from what you know to be “normal” for you, it is unwise to continue repeating that activity over and over (do what you have to do for competition though). Not only are you ingraining less efficient movement patterns, but in the brain, you are associating threat with that activity after every rep, which digs a deeper hole which you’ll have to climb out of. There are surely other exercises or training modalities that can be incorporated to get the same or similar training stimulus.
- Similar to the Q-angle discussion above, as a coach, be cautious about “demonizing” certain biomechanical positions with regards to PFPS and other chronic pain syndromes, especially if the athlete is not currently in pain. For example, say you have an athlete or client whose knees tend to dive into a valgus state upon running, jumping, squatting, etc. Yes, we want to correct it, but I would avoid such statements as, “we have to fix that, or your knees are going to hurt/you could get injured.” Based on findings so far, such a statement may or may not actually be true, depending on the type of athlete and desired activity (at least as far as PFP goes). What that statement does, without a doubt, is associate fear and threat with a particular movement. Of course, we absolutely want to coach and correct positions. We will talk more about the importance of coaching later. It’s very important. However, make the cueing a little more positive. Example – “we are fixing this because it is a safer and more stable position for you to generate force.
- If there was ever a client population that needed to be watched closely regarding positions and mechanics, it seems to be adolescent (middle and high school) female athletes. The lack of hip/core/trunk/foot (probably all of it) control in this population seems to lend itself well to a greater risk of PFP.
- Altered Neuromuscular Control of The Hip and Knee
So, if PFP is associated with altered movement mechanics during activities such as squatting, running, and jumping, it would make sense to see differences in the function of the muscles that control those movements, compared to healthy individuals. We definitely see that, but again, with several different trends. Examples include:
- Females with PFP consistently demonstrate decreased hip external rotation, and abduction isometric strength measured, in both active and inactive populations
- Males with PFP tend to demonstrate decreased knee extensor isometric strength
- Decreased hip abduction isometric strength was associated with increased knee valgus moments during running, which increased with fatigue.
- Delayed glute medius function during a step up activity
- Hip abduction weakness + increased hip abductor EMG activity during an eccentric step down exercise
- Decreased hip extension strength, but yet increased EMG activation of glute maximus during running and step down exercises, compared to healthy controls.
- Distal quadriceps neuromuscular control showed similar alterations, but to a lesser extent.
It makes intuitive sense that if knee valgus is a common mechanical fault in the dynamic movement patterns of those with PFP, then there would be weakness in the muscles that oppose it. So, it is no surprise we see weakness of the hip external rotators and abductors.
However, strength of these muscles groups was tested in an open chain fashion, such as in the pictures below.


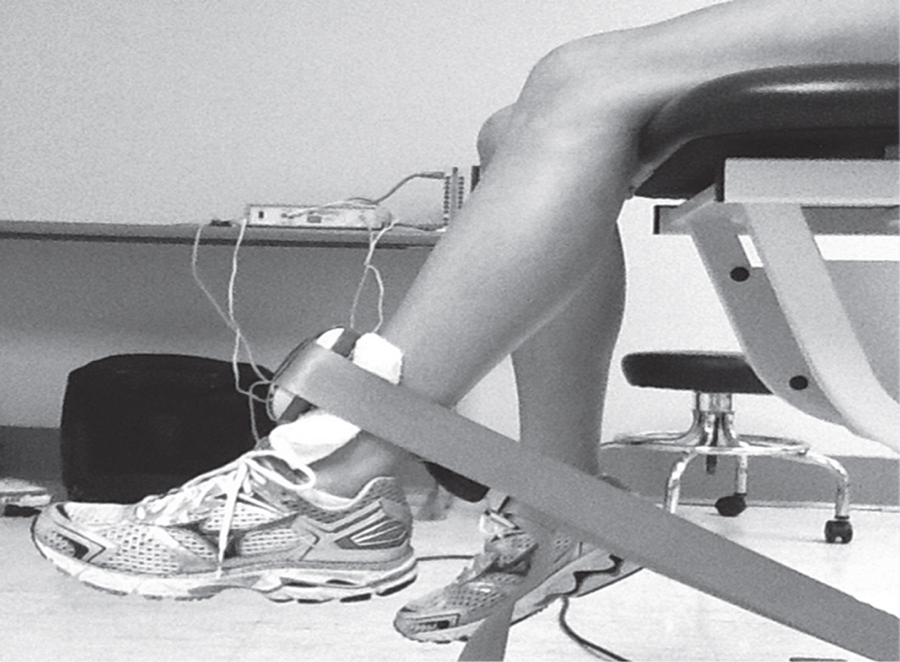
This type of voluntary maximum isometric testing does not necessarily mimic the involuntary reflexive demands of these muscle groups during closed chain activities such as squatting, stepping, and jumping activities. This may explain inconsistencies in the research regarding the associations between muscle weakness and movement patterns. Some studies did show association as described above; but others showed such variations as participants having weak hip abductors but not necessarily demonstrating lack of control in the frontal plane, or showing weakness with hip external rotation but not demonstrating abnormal motion in the transverse plane during dynamic activity. So even though all participants with PFP demonstrated weakness in at least one plane of motion, was testing strength in this fashion really getting to the root of the problem, or was it just picking up pain inhibition? Again, chicken or egg.
Based on a systematic review done last year of the available literature on the topic, maximal isometric hip strength was NOT a risk factor for PFP. In other words, the weakness that we see in isometric hip strength with those (females especially) who have PFP, is more likely due to the pain itself (a symptom); rather than a contributing cause of the PFP response.
What I thought was pretty interesting, however, was that muscle groups that typically tested weak actually showed higher EMG activity during dynamic movements versus healthy individuals. The hypothesis here was that weak muscles were working overtime to try to stabilize and perform the movement. This is consistent with what the great Charlie Weingroff says about EMG – “It doesn’t lie, but it doesn’t tell the whole story”. He uses the example of comparing two people who’s max back squats are both 500lbs. He’s taking the guy who has less EMG activity in the abdominals, as this indicates he is expending less energy and likely has more movement options at his disposal. There was also evidence of delayed timing of certain muscles groups, which seems to hit closer to the root of the issues – reflexive neuromuscular control. Unfortunately, there is little in the way of prospective studies (looking for risk factors) regarding reflexive neuromuscular control
**Take Home Points**
- There is clearly some kind of neuromuscular component to PFP.
- Weakness in one plane was not always associated with altered movement in that same plane, based on how the researchers measured strength. However, that doesn’t mean compensations were not there, it just means they may have happened somewhere else, and were not measured. Make sure you are paying attention to what’s going on at the foot, pelvis, and trunk, as compensations can hide in those places. For example, if one’s hip abductors are not stabilizing correctly in a single leg activity, they athlete may shift his or her body weight laterally through the pelvis in order to balance; or collapse through the arch of the foot in an effort to create more ground contact. In fact, these are compensation patterns that the researchers observed during testing, they were just not equipped to measure and verify it.
- The ability to create voluntary muscular force is much different than the reflexive timing and stabilization capacity needed of a muscle group during weight-bearing activities.
- Intervention
So, to recap thus far, PFP is:
- Typically under or around the knee cap during weight-bearing movements with a flexed knee – running, squatting, step-ups/stairs, jumping, and landing.
- Associated with isometric weakness of the hip in various planes (especially females), and of the distal quadriceps (more so in males) – when PFP is already present
- Associated with altered neuromuscular control of those same muscle groups when PFP is already present.
- Associated with altered kinematics at the foot, knee, hip, and/or trunk during dynamic activity.
So what do we do about it?
Hip & Quad Strengthening In The Open Chain
Since weakness of the hips and distal quads was present in many of the participants with PFP, several studies have incorporated strengthening protocols. Some of those protocols involved only exercises that looked like this, being performed at 3 sets of 10 repetitions. The classic, “glute activation” protocol.
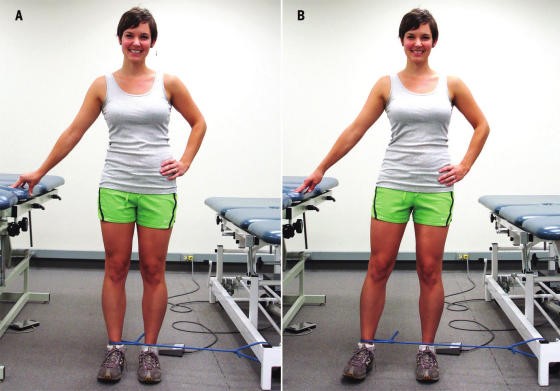
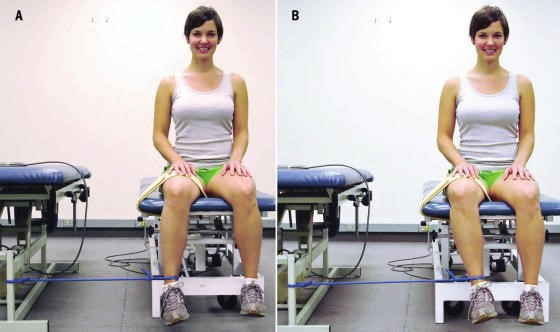

You are probably laughing. “Typical PT garbage”. How are these worthless open chain exercises going to strengthen muscles or affect a condition that is present in weight bearing patterns? I’m with ya. Except that in pretty much every study, the participants demonstrated greater hip strength and reported less pain! Before we deem it a miracle, let’s talk about it. In many of the papers incorporating these basic exercises, the participants were either sedentary or were recreational runners. So, in other words, they were probably very weak, and these exercises were enough to give them a stimulus and subsequent strength adaptation. The strength testing was in the open chain and the exercises were in the open chain; so that explains the carryover.
However, some of the programs implementing these types of things were only 3-4 weeks long. This is not enough time to develop appreciable hypertrophy to explain the increase in force production. The likely explanation here is these exercises improved neuromuscular signaling, so that the participants were better able to recruit motor units and demonstrate the strength that they already possessed. Would a group of highly trained individuals with PFP have responded to the exact same basic protocols as favorably? Hard to say, but probably not.
What these exercises did not do was change mechanics or neuromuscular timing during dynamic weight-bearing activities. This is not surprising. So then, how did they help to decrease the patient’s pain? The actual mechanism? We don’t know. There’s always the argument that untrained or recreational-only individuals were simply doing something different that they thought would work, and so it did. Perhaps, by increasing neural drive to the muscles of the hips, regardless of the nature of the activity, this decreased the threat response in the brain – which subsequently decreased pain perception. Like the brain said, “hey things can actually fire down there, so maybe our legs aren’t actually going to fall off every time we go up and down the stairs.” Perhaps the movement variability that the exercises provided gave enough proprioceptive input to the brain that it made all lower extremity activities less threatening, regardless of mechanics. Maybe the “feel-good” hormones that were released with exercise also helped to quell the perception of pain. I would have liked these studies to compare to some type of sham treatment.
The use of hip strengthening techniques like the ones above seem to be superior for reducing symptoms when compared to open chain quadriceps strengthening. Quad exercises included: straight leg raises, quad sets, short arc quads, and knee extensions. Those performing these exercises alone also improved, just not to the same extent. And like the open chain hip activities, these basic quad exercises did nothing to alter or improve what were thought to be faulty mechanics during dynamic activity.
Hip & Quad Strengthening In The Closed Chain
There were also studies that incorporated closed chain strengthening such as variations of squatting, lunges, step up, step downs, single leg hinges balance, etc. The studies had a mix of untrained and trained participants. The participants reported less pain after these more intense regimens as well. They also demonstrated improved hip strength and kinematics during various dynamic activities! Sounds like we have a winner! The issue is that the participants in these studies were also coached through proper biomechanics during the exercises. This is great for real world validity, but it confounds things a bit; as maybe these more complex movement patterns require the proper coaching in order to be effective. Of course this is not necessarily a negative; because if 2 or 3 sessions of movement coaching will yield similar improvements as going to the clinic 3x/week for 6 weeks, I choose the former, with a maintenance corrective program.
For the running population, coaching seems to be very effective for improving mechanics and subsequently reducing PFP. They simply cued for symmetry of stride, a relatively level pelvis, forefoot strike, and knees tracking over feet. A mirror was also used, so that the athlete could see what was going on. No banded hip exercises needed, or an intense regime of closed chain exercises. Now, those things could definitely be a part of the home exercise program, but on the client’s time.
Then there was the “multi-modal” studies. Basically this means that the participants performed several different flexibility and strengthening exercises, utilized taping techniques, and received various manual therapy techniques. They got better too; but because they used every intervention under the sun, we don’t know what worked.
Muscle flexibility was something that was looked at by only a few studies that I saw, but is commonly addressed with PFP. Muscles commonly thought to be “tight” and contributors to PFP are calves, quads, hip flexors, etc. It is difficult to objectively quantify these things in studies, which is probably why they were not included very often. Clinically, I do a whole lot of cranking on people. If they want to do some light stretching on their own, that’s typically fine; but we generally get way more bang for our buck looking at other things.
Finally, the use of physical agents (therapeutic modalities) has not shown benefit in patients with PFP compared with controls. Here is a quote from a systematic review:
“None of the therapeutic modalities reviewed (ultrasound, iontophoresis, phonophoresis, neuromuscular electrical stimulation, EMG feedback, TENS, laser) has sound scientific justification for the treatment of PFPS when used alone.”
I will simply say that this comes as no shock.
Summary
I started this Part I article by saying the cause of PFP is multifactorial. Combinations of biomechanical, neuromuscular, and autonomic (nociception and pain perception) are all likely contributing factors. The nature of the treatment seems to be the same. We first need to eliminate the aggravating activities if the PFP is causing you to compensate in some way. This does not mean stop training. It means find something else that does not flare you up. Then we address movement patterns. This may be through simple cueing, or may be done by regressing the activity to its subsequent parts, and building positions from the ground up. Drills and neuromuscular tricks can be incorporated to increase the neural drive where we want it, based on the movement pattern that we are trying to build back up.
In Part 2, we shall go through a sample protocol outlining all of this.
Related Articles
[Strong360] Improving Movement Quality
Dealing with Knee Pain (Video) Training Around Injuries Quinn Henoch has a Doctorate of Physical Therapy from the University of Indianapolis. He is the head of rehabilitation for Darkside Strength and Core Sports Performance in Louisville, KY. He also works for the Kentucky Orthopedic Rehab Team managing orthopedic and sports related dysfunction. Quinn played football at the Div 1-AA level at Valparaiso University as a defensive back. He has also competed in track and field, Crossfit, and powerlifting. Currently, he trains full time as an Olympic weightlifter, and is a 2014 American Open qualifier in the 77kg classWebsite, Facebook, Twitter
Witvrouw E, Callaghan MJ, Stefanik JJ, et al. Patellofemoral pain: consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver, September 2013. Br J Sports Med. 2014;48:411–414.
Dierks et al. Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. JOSPT. Vol 38(8)Aug 2008
Dierks et al. Lower extremity kinematics in runners with patellofemoral pain during a prolonged run. Med Sci Sports Exerc. 2011 Apr;43(4):693-700
Khayambashi et al. The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain: a randomized controlled trial. JOSPT. Jan 2012 Vol 42(1)
Ferber et al. Changes in knee biomechanics after a hip-abductor strengthening protocol for runners with patellofemoral pain syndrome. Journal of Athletic Training. 2011;46(2):142-149
Bolgla et al. Comparison of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome. JOSPT. Vol 6(4) Dec 2011
Herbst et al. Prospective hip and knee strength measures associated with increased risk for patellofemoral pain incidence. OJSM. July 2014 2(2).
Noehren et al. Prospective evidence for a hip etiology in patellofemoral pain. Medicine and Science in Sports and Exercise. 2013 45(6)
Khayambashi et al. Posterolateral hip muscle strengthening versus quadriceps strengthening for patellofemoral pain: a comparative control trial. Physical Medicine and Rehabilitation. May 2014 Vol 95(5)
Myer et al. High knee abduction moments ar common risk factors for patellofemoral pain (PFP) and anterior cruciate ligament (ACL) injury in girl: is PFP itself a predictor for subsequent ACL injury? Br J Sports Med. 2015; 49:118-122
Rathleff et al. Is hip strength a risk factor for patellofemoral pain? A systematic review and meta-analysis. Br J Sports Med. 2014; 48:1088(10)